It’s one of the most important questions in prostate cancer care: How can a modern multi-parametric magnetic resonance imaging (mpMRI) scan miss cancer?
mpMRI is a non-invasive imaging technique that uses magnetic fields to generate detailed images of soft tissues inside the body, without using radiation. The “multiparametric” designation means the scan combines several different imaging sequences, typically including diffusion-weighted imaging, dynamic contrast enhancement, and T2-weighted imaging, to characterize tissue in multiple ways simultaneously, which improves the ability to detect suspicious lesions.
For most men today, the journey toward a prostate cancer diagnosis begins with something simple: an elevated prostate-specific antigen (PSA) level or an abnormal digital rectal examination. The next step is usually an mpMRI scan. When the scan lights up a suspicious lesion, the path forward is clear: a targeted biopsy, often combined with systematic sampling. But what happens when the mpMRI scan appears to be clean?
Recent studies have shown that the mpMRI’s negative predictive value (NPV), meaning the probability that a negative scan truly rules out clinically significant cancer, is typically 74-85%. That means that up to one in four men with a “negative” MRI could still harbor clinically significant prostate cancer. That is why confirmatory biopsies are increasingly common even after a clear MRI.
In an ongoing project at Northwestern Memorial Hospital, our team wanted to understand why some prostate cancers remain invisible on mpMRI, and what is happening in the tissue itself that keeps the cancer hidden? We are currently preparing a complete scientific manuscript with our full dataset and analysis. Here, we illustrate the key concepts using a representative case.
Looking Inside the Invisible Lesions
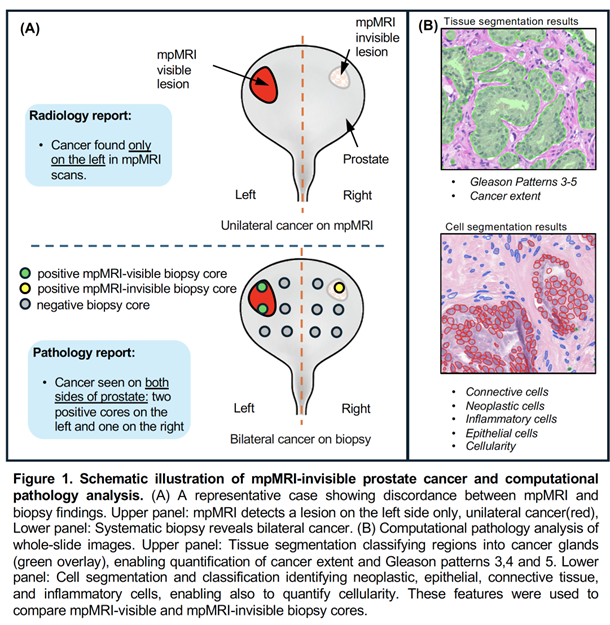
We studied patients who had a lesion detected on mpMRI on only one side of the prostate (unilateral), but whose subsequent biopsy revealed cancer on both sides (bilateral). To illustrate this concept, Figure 1A shows a schematic example of this scenario: mpMRI identifies a suspicious lesion on one side of the prostate, while the other side appears normal on imaging, yet biopsy confirms cancer is present on both sides. We categorized biopsy cores into two groups: those taken from the mpMRI-detected lesion (“mpMRI-visible biopsies”) and those taken from the opposite side where mpMRI showed no lesion (“mpMRI-invisible biopsies”).
Using a computational pathology workflow, we performed tissue- and cell-level analyses of high-resolution whole-slide images (WSIs). This approach allowed us to map cancerous glandular structures and cellular composition in a systematic and interpretable way. We quantified key features from WSIs, including cancer extent, glandular architecture, and cellular density, to compare mpMRI-visible and mpMRI-invisible biopsy cores (Figure 1B).
Insights from the Tissue
We found that lesions that appeared on MRI generally exhibited:
- Greater tumor extent, meaning larger, more continuous areas of cancer within the biopsy core
- Higher cellularity, meaning more densely packed neoplastic cells within the tissue.
Tumor grade (Gleason patterns) did not independently predict mpMRI visibility. In other words, the size and density of the tumor appear to influence detection more than its histologic grade.
MRI relies on tissue contrast and water diffusion to generate images. Tumors with higher cellularity composed of neoplastic cells restrict water movement more, producing stronger MRI signals. Tumors that contain dispersed neoplastic cells or contain more stromal tissue may blend with normal prostate tissue, making them less conspicuous on imaging.
This does not indicate a shortcoming of MRI; rather, it reflects the natural variability of tumor biology. Understanding these tissue-level differences provides context for interpreting imaging results and may help enhance imaging protocols.
Author:

Ramin Nateghi
Postdoctoral Scholar
Northwestern University, Feinberg School of Medicine, Chicago, IL, USA
LinkedIn: https://www.linkedin.com/in/ramin-nateghi/
1 comment(s) on "When Multi-Parametric Magnetic Resonance Imaging (MRI) Cannot See: What Pathology Reveals About “Invisible” Prostate Cancer"
05/19/2026 at 05:50 PM
Michele Mitchell says:
Fascinating article! I hope you publish your findings- it can help so many patients! Well done!Please log in to your DPA profile to submit comments